What is Childhood Apraxia of Speech
By Sara Baines-Miller | Posted on: June 12, 2019
What is Childhood Apraxia of Speech?
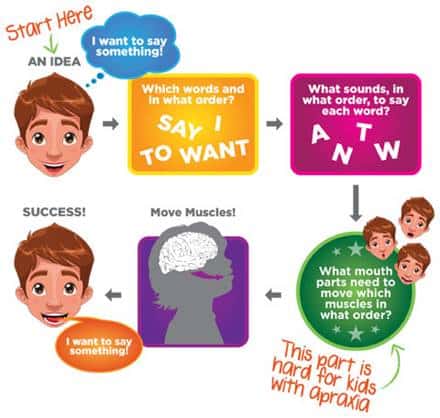
Childhood apraxia of speech (CAS) is a label for a motor speech disorder in which a child’s brain has difficulty determining how and when to move the jaw, lips, and tongue to produce speech.
In essence, the brain has difficulty planning, writing and implementing directions to the muscles in order to tell them how and when to move.
Children with CAS are at high risk for developing difficulties with literacy (reading/writing) problems as a result of underlying difficulties with phonological and phonemic awareness skills (i.e., how to notice, think about and work with the sounds in words and spoken language).
Children with CAS typically have much higher receptive (understood) language than expressive (spoken) language due to difficulties with speech production.
CAS is typically present from birth, but can also result from a neurological event (e.g., stroke, brain injury, etc.). It appears to affect more boys than girls.
When CAS is present in a deaf or hard of hearing children, it adds an extra layer of difficulty for them in learning how to speak.
At DePaul School for Hearing and Speech, we have worked with many students who possess both hearing loss and CAS. Using a modified listening in spoken language and a motor-based intervention, we are able to help these children improve their spoken language skills.
In this blog post, we are going to cover the basics of CAS including an overview, signs, and treatment options to better understand this disorder.
Childhood Apraxia of Speech Overview
A child with CAS knows what he/she wants to say, however there seems to be a disconnect between a child’s brain and their ability to move their mouth to carry out the word or sentence.
The speech muscles aren’t “weak.” Rather, they don’t perform as they should because the brain struggles to coordinate the associated movements needed to carry out the words. This includes the five parameters of movement: range of motion, direction, speed, force, and tension.
Though CAS is typically a developmental disorder, children do not grow out of it alone and will require professional intervention with a trained speech-language pathologist.
Treatment, which we will cover later in this blog, is necessary to treat the underlying problems present in CAS in order to improve the child’s speech.
Signs of Childhood Apraxia of Speech
The signs of CAS can vary depending on their age. They include but aren’t limited to:
- 18 months – 2 years: Delayed use of first words, limited vocabulary (not receptively but expressively), or the ability to form only a handful of consonant/vowel sounds.
- 2 – 4 years: Consonant/vowel distortions, pauses between syllables.
The signs of this disorder can be mild or severe depending on the child’s case.
Severity of apraxia is not judged by the severity of the speech errors, but by how easy/hard it is to cue a child to correct his/her speech
Other more prominent signs and symptoms of CAS include:
- Limited babbling
- Issues with feeding as an infant
- Discoordination of fine and gross motor skills
- Difficulty carrying over and generalizing skills that are learned
- Syllable segmentation that may be fast or slow (ex: ha-ppy vs. happy)
- Inconsistent production of vowel sounds (This is a hallmark of CAS)
- Inconsistencies of productions of the same word across multiple trials
- Greater difficulty producing longer words/phrases
- Awkward or clumsy movements from one sound to another
- Groping or trial-error behavior when producing speech
- Distortions that aren’t necessarily substitutions of intended C’s and V’s
- Adding extra sounds in words/syllables
- Distortions of consonants/vowels
Treatment for Childhood Apraxia of Speech
There are many types of speech therapies that are available to treat CAS. The overall goal is NOT to help improve your child’s specific sound production, but the overall coordination, movement, and gestures for speech.
For example, a child with CAS will practice one sound at a time.
Typically, therapy begins with your child’s speech-language pathologist focusing on practicing phrases, syllables, and words.
However, it’s suggested that therapy begins at “syllable level” using consonants/vowels that are already present in the child’s repertoire so they have success early in therapy.
Target selection should be thoughtful and customized to the child’s abilities and difficulties.
A speech-language pathologist will use the Principles of Motor Learning and motor-based, multi-sensory approach (visual, tactile, auditory, etc.) during speech therapy.
Therapy also includes:
- Speech drills that will require your child to correctly repeat therapy targets. Perfect practice makes perfect.
- Practicing the formation and pronunciation of sounds within the context of meaningful words and syllables (NOT in isolation unless absolutely necessary to achieve correct placement)
- Practice prosody (the melody of speech) to instill flexibility in the motor plans and natural sounding speech later (say it angry, say it sad, say it happy) so you don’t get telegraphic speech)
Repetition and frequency of practice are major factors in treatment success. Frequent and intense intervention is required. The gold standard is 10, 30-minute sessions per week or at least five, 30-minute sessions if tolerated.
For more information on how DePaul School for Hearing and Speech works with students that are both hard of hearing and have CAS, please click here.
Share This Article: